

Volume 22, Issue 6 (February & March 2020)
J Arak Uni Med Sci 2020, 22(6): 288-295 |
Back to browse issues page




![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadighi A. Subcutaneous Emphysema Following Molar Tooth Extraction: A Case Report. J Arak Uni Med Sci 2020; 22 (6) :288-295
URL: http://jams.arakmu.ac.ir/article-1-6158-en.html
URL: http://jams.arakmu.ac.ir/article-1-6158-en.html



Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Khorasgan Branch, Islamic Azad University Isfahan, Iran. , arsadighi@gmail.com
Full-Text [PDF 1983 kb]
(1048 Downloads)
| Abstract (HTML) (4678 Views)



Full-Text: (4012 Views)
Extended Abstract
Introduction
The surgical extraction of third molars is the most frequent surgical procedure in oral surgery. Complications may occur despite the skill and experience of surgeon. Subcutaneous emphysema is an uncommon clinical condition caused by forceful injection of air into the loose connective tissue below the dermal layer, and mostly is the result of using a high-speed air-driven hand piece during surgical tooth extraction. The aim of this article is to report a case of the subcutaneous emphysema created molar tooth extraction in a patient and its treatment.
Case Report
This study is a case report of subcutaneous emphysema occurred during the right third molar extraction (in the horizontal position, near the mandibular canal) by using an air-driven hand piece in a 28-year-old female patient referred to Kashani Hospital, Isfahan, Iran. The patient, complaining of swelling and pain in the right side of her face, acknowledged that the swelling was almost immediately during surgery.
Results
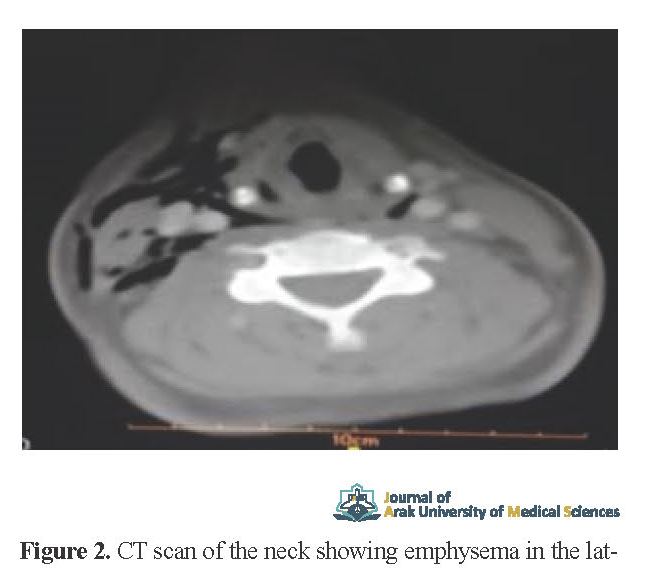
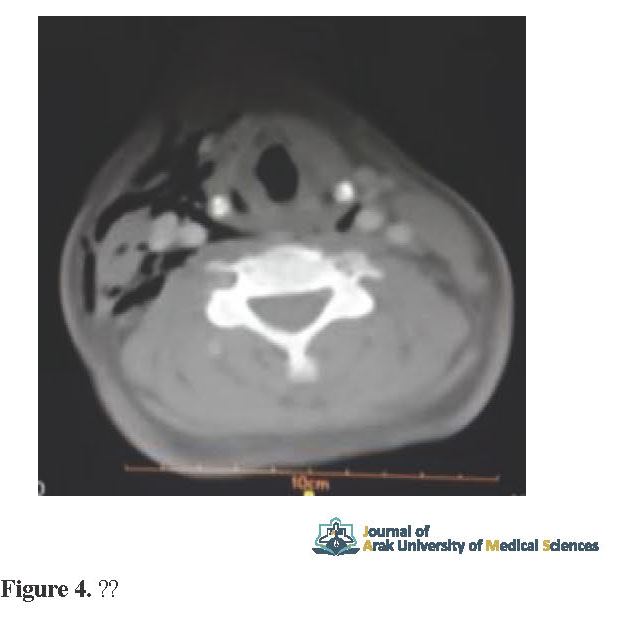
In the clinical examination of crepitation and sensitivity in the right side of the face, the right carotid triangle extended to the right clavicle was observed. Trismus was present with maximum opening of about 30 mm (Figures 1, 2, and 3), and no signs of dysphagia and dyspnea were reported. The patient's blood pressure was 125.65, heart rate 73 and body temperature 37.3. Arterial oxygen saturation was reported 94%. Patient was administered 4 million units of penicillin Intravenous (IV) every 4 hours, metronidazole 500 mg IV every 8 hours solved in 100 cc normal saline infused slowly, and rinsing mouth with 0.2% chlorhexidine every 8 hours. On CT, it was observed that emphysema was spread to the right subcutaneous areas, lower eyelid, buccal, submandibular salivary glands lie under the side of the jaw, the back of the neck around the carotid sheath, chest wall and mediastinum (Figure. 4, 5, 6). The patient was hospitalized for 36 hours and treated with antibiotic regimen and monitored with no respiratory distress or pain. Following a decrease in swelling, maximal opening of the mouth by more than 30 mm became possible. Then, she was followed up for day 5 until complete resolution of swelling, maximum opening up to 50 mm, and lack of crepitation. No other local, systemic and infectious complications occurred.
Introduction
The surgical extraction of third molars is the most frequent surgical procedure in oral surgery. Complications may occur despite the skill and experience of surgeon. Subcutaneous emphysema is an uncommon clinical condition caused by forceful injection of air into the loose connective tissue below the dermal layer, and mostly is the result of using a high-speed air-driven hand piece during surgical tooth extraction. The aim of this article is to report a case of the subcutaneous emphysema created molar tooth extraction in a patient and its treatment.
Case Report
This study is a case report of subcutaneous emphysema occurred during the right third molar extraction (in the horizontal position, near the mandibular canal) by using an air-driven hand piece in a 28-year-old female patient referred to Kashani Hospital, Isfahan, Iran. The patient, complaining of swelling and pain in the right side of her face, acknowledged that the swelling was almost immediately during surgery.
Results
In the clinical examination of crepitation and sensitivity in the right side of the face, the right carotid triangle extended to the right clavicle was observed. Trismus was present with maximum opening of about 30 mm (Figures 1, 2, and 3), and no signs of dysphagia and dyspnea were reported. The patient's blood pressure was 125.65, heart rate 73 and body temperature 37.3. Arterial oxygen saturation was reported 94%. Patient was administered 4 million units of penicillin Intravenous (IV) every 4 hours, metronidazole 500 mg IV every 8 hours solved in 100 cc normal saline infused slowly, and rinsing mouth with 0.2% chlorhexidine every 8 hours. On CT, it was observed that emphysema was spread to the right subcutaneous areas, lower eyelid, buccal, submandibular salivary glands lie under the side of the jaw, the back of the neck around the carotid sheath, chest wall and mediastinum (Figure. 4, 5, 6). The patient was hospitalized for 36 hours and treated with antibiotic regimen and monitored with no respiratory distress or pain. Following a decrease in swelling, maximal opening of the mouth by more than 30 mm became possible. Then, she was followed up for day 5 until complete resolution of swelling, maximum opening up to 50 mm, and lack of crepitation. No other local, systemic and infectious complications occurred.

Discussion
Subcutaneous emphysema is seen mostly in the third and fifth decade of life and in the right mandibular wisdom tooth extraction surgery site. Emphysema can spread to deep spaces such as infratemporal, pterygomandibular, masseteric, lateral or retropharyngeal or mediastinum [6]. Differential diagnoses in this case may include allergic reactions to drugs, hematoma, angioedema, and infection [4, 9, 10]. Emphysema is an uncommon condition in oral health and mostly is the result of using a high-speed air-driven handpiece during surgical tooth extraction [11, 12]. A review of studies in which 32 cases of subcutaneous emphysema were investigated showed that half of the cases involved the use of air-driven hand pieces [12]. The retropharyngeal space, also called the potential space, has the ability to transmit air to the dorsal mediastinum. The involvement of the lateral and pharyngeal spaces may block the airway, so their careful monitoring is necessary. In some cases, the orbital space is compressed by the air and subsequently the optic nerve is injured [4]. In most cases, subcutaneous emphysema begins after days 3 to 5, and is then fully managed within 7 to 10 days [12]. It is important to advise patients to avoid increasing pressure inside the mouth, for example, by heavily nose blowing or playing wind instruments [16]. Emphysema can be prevented by following routine surgical procedures. The height of the periosteal mucosal flap should be minimal and should not extend to the alveolar lingual segment of the third mandibular molar. Moreover, the duration of the use of air-driven high-speed handpieces should not be excessive, or even be replaced by the multiplier contra-angle 1: 5 handpieces, which does not use high-speed airflow for movement.
Subcutaneous emphysema is seen mostly in the third and fifth decade of life and in the right mandibular wisdom tooth extraction surgery site. Emphysema can spread to deep spaces such as infratemporal, pterygomandibular, masseteric, lateral or retropharyngeal or mediastinum [6]. Differential diagnoses in this case may include allergic reactions to drugs, hematoma, angioedema, and infection [4, 9, 10]. Emphysema is an uncommon condition in oral health and mostly is the result of using a high-speed air-driven handpiece during surgical tooth extraction [11, 12]. A review of studies in which 32 cases of subcutaneous emphysema were investigated showed that half of the cases involved the use of air-driven hand pieces [12]. The retropharyngeal space, also called the potential space, has the ability to transmit air to the dorsal mediastinum. The involvement of the lateral and pharyngeal spaces may block the airway, so their careful monitoring is necessary. In some cases, the orbital space is compressed by the air and subsequently the optic nerve is injured [4]. In most cases, subcutaneous emphysema begins after days 3 to 5, and is then fully managed within 7 to 10 days [12]. It is important to advise patients to avoid increasing pressure inside the mouth, for example, by heavily nose blowing or playing wind instruments [16]. Emphysema can be prevented by following routine surgical procedures. The height of the periosteal mucosal flap should be minimal and should not extend to the alveolar lingual segment of the third mandibular molar. Moreover, the duration of the use of air-driven high-speed handpieces should not be excessive, or even be replaced by the multiplier contra-angle 1: 5 handpieces, which does not use high-speed airflow for movement.
Ethical Considerations
Compliance with ethical guidelines
This study has no specific ethical considerations. A written informed consent was obtained from the patient to use her information and images.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors declare no conflict of interest.
Compliance with ethical guidelines
This study has no specific ethical considerations. A written informed consent was obtained from the patient to use her information and images.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors declare no conflict of interest.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
